Home
+

Published : 21 Oct 2024, 02:15 AM
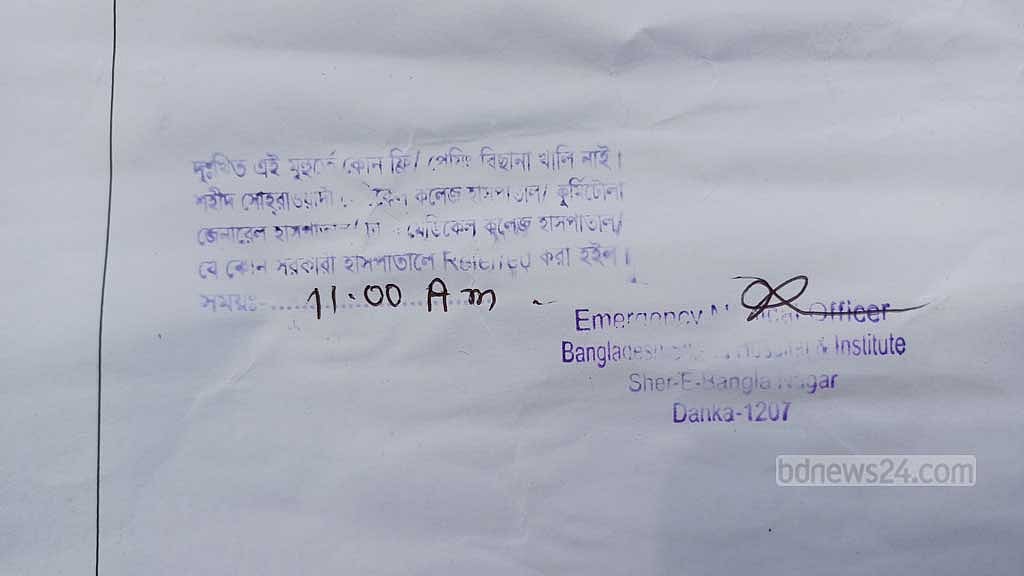
Tawsin Ahmed had been suffering from pneumonia. His parents took the 1-year-old child from Cumilla’s Barura to Dhaka but were forced to return home after failing to secure a hospital bed.
Tawsin was rushed to the Bangladesh Shishu Hospital and Institute in Agargaon, where emergency department doctors diagnosed him with pneumonia and recommended admission.
The hospital had no available beds equipped with oxygen support, and they stamped his prescription with the note, “Sorry, there are currently no free/paid beds available.”
The child was then referred to Shaheed Suhrawardy Medical College and Hospital, Dhaka Medical College Hospital, Kurmitola General Hospital, or any other government hospital.
Tawsin’s father, Abdur Razzak, shared the traumatic experience with bdnews24.com. “The doctor said his condition is not good. They suggested admitting him, but there are no beds available here [Shishu Hospital]. We visited two more hospitals, and they also said there were no vacant beds.
He added, “It is difficult for us to afford treatment in private hospitals in Dhaka, so we are returning to Comilla for treatment.”
According to government statistics, pneumonia claims the lives of around 24,000 children annually in the country, averaging over 65 deaths per day.
The 2022 Demographic and Health Survey revealed that pneumonia is responsible for the deaths of 24 out of every 100 children under the age of five.
Children require oxygen support when their condition worsens. However, the number of such beds is limited in district hospitals, forcing patients to be referred to larger cities like Dhaka.
The high patient influx makes securing a bed difficult. The financial strain on families unable to secure hospital beds can be overwhelming.
When beds are unavailable in government hospitals, the financial burden on the patient's family becomes difficult to manage.
Not only pneumonia, but many other childhood illnesses also require oxygen support for treatment. However, adequate facilities are lacking in Upazila, district, and divisional hospitals.
As a result, countless parents, like Tawsin's, navigate from hospital to hospital each day. Children cry, and sometimes their cries fall silent forever.
Parents' frustration transforms into anger. However, obtaining clear information from authorities about visible actions or specific plans to address these deficiencies in the healthcare infrastructure is challenging.
From Sept 21 to Oct 17, the Bangladesh Shishu Hospital and Institute referred 1,200 children to other hospitals due to bed shortages.
The actual figure may be higher, as many patients cannot be registered when the hospital is under pressure. At least 90 percent of these children required oxygen.
This 680-bed facility has 18 Newborn Intensive Care Unit, or NICU, beds, 18 Pediatric Intensive Care Unit, or PICU, beds, 18 High Dependency Unit, or HDU, and isolation beds, and 361 beds equipped with oxygen support, but it is insufficient to manage the situation.
Mahmudul Haque Chowdhury, a resident doctor in the hospital’s emergency department, told bdnews24.com: “We can admit one child per bed. As long as there are vacancies, we can admit patients. However, many more children arrive at our hospital, and we refer them to other government facilities.”

IN SEARCH OF A LITTLE OXYGEN
On Oct 1, 1-year-old Omar, known only by his single name, suffering from pneumonia, was brought to the Bangladesh Shishu Hospital and Institute from Razapur in Bhola Sadar Upazila.
He had been admitted to Sher-E-Bangla Medical College Hospital in Barishal on Sept 25.
With no beds available at the children's hospital, Omar was taken to Dhaka Medical College Hospital, where his condition was critical, suffering from severe respiratory complication and malnutrition.
However, there were no available beds at this hospital either. The family faced further disappointment after reaching out to several other hospitals in Dhaka.
Omar was eventually taken to a private hospital in Shyamoli, though his family struggled to afford the cost of treatment.
Omar’s grandfather, Hasmat Ullah, told bdnews24.com: "The ambulance fare was Tk 7,000, but could not pay the full amount. Now we do not know how we will manage the hospital bills.”
After being treated at City General Hospital for two days, Omar was slightly better, and his family decided to take him home on Oct 10.

HOSPITAL TO HOSPITAL VISITS BECOME A ‘FATE’
Most children referred from the Shishu Hospital are directed to the pediatric ward of Shaheed Suhrawardy Medical College Hospital. Some are admitted, but most are turned away due to overcrowding.
Wards 314 and 313 remain packed year-round. Each bed accommodates multiple children, with parents needing to stay close by. The congestion makes movement nearly impossible.
Hasna Hena from Dhaka’s Keraniganj had to take her 4-year-old daughter, Jannatul Ferdousi, from the Shishu Hospital to Shaheed Suhrawardy Medical College Hospital.
Though she managed to get a bed, she expressed concern after seeing the condition in the ward.
"The doctor says she [Jannatul] needs to be admitted urgently; due to fever, she has a urinary infection and pneumonia. They referred us here without admission. We got a bed, but there is no room to move," said Hena.
Shahnaz Begum, a mother from Rupganj in Narayanganj, arrived at Shaheed Suhrawardy Medical College Hospital with her child, Sajid Hossain.
She said,"I spent two days running around the Shishu Hospital but could not admit him. His condition became serious, so we brought him here. I see two children on one bed; now they have put three.”
A father from Mirpur brought his 2-year-old child, suffering from severe respiratory distress, from a private hospital to Shaheed Suhrawardy Medical College Hospital.
He kept his child in the ambulance with oxygen while he rushed to ward 313. The private hospital had advised him to admit the child to an ICU.
“I brought him in an ambulance with four litres of oxygen. He needs urgent admission, but we could not get him into the Shishu Hospital,” the father said.
Upon reaching the Shaheed Suhrawardy Medical College Hospital, his anxiety increased. Doctors advised him to transfer the child to Dhaka Medical College Hospital or another hospital due to the absence of ICU facilities.

A doctor from Ward 313, speaking on the condition of anonymity, said there are 20 beds in their unit, but they often have 60 to 70 children admitted.
“We can provide treatment for children with pneumonia or respiratory issues using normal oxygen support. We often have three children per bed. If more come, we refer them elsewhere. We cannot admit children requiring ICU or ventilation,” he said.
Shaheed Suhrawardy Medical College Hospital does not have a central oxygen supply; instead, oxygen is administered via cylinders.
Parents of children who cannot be admitted at Suhrawardy Hospital often head to Dhaka Medical College Hospital, where Ward 208 handles pediatric cases.
There, two children with nasal tubes are seen lying on the same bed while another child is held by its mother, also receiving oxygen.
Each bed in the ward accommodated three children, and some were even placed on mattresses on the floor. Many of these children were suffering from pneumonia or other respiratory issues.Unit-1 of the pediatric department has two sections: one with 23 beds holding 60 children and another with 14 beds accommodating 57 children.
In Unit-2, doctors reported having to admit 70 to 100 children into 19 available beds.
Prof Lutfan Nessa, the chair of the pediatric department, shared her challenges with bdnews24.com.
“We typically do not turn patients away, but we often have three patients per bed and two on the floor. We sometimes have to admit five children per bed.
“Such situations arise, and we struggle to provide the services we wish to offer. While we are providing care, it has become increasingly difficult for us,” she said.
WHICH CHILDREN REQUIRE ARTIFICIAL OXYGEN?
Paediatric specialist Prof Mohammad Shahidullah told bdnewsews24.com that 90 percent of children requiring oxygen in hospitals suffer from pneumonia, bronchiolitis, and acute respiratory complications.
The remaining 10 percent need oxygen due to respiratory issues caused by other illnesses.
"For regular respiratory distress, children are given oxygen. However, when the condition becomes severe, supplemental oxygen alone cannot meet their needs, and a higher level of support, such as ventilation, becomes necessary," he added.

TRAPPED BY PRIVATE HOSPITAL BILLS
When access to government hospitals is unavailable, parents are left with no choice but to turn to private facilities, often leading to financial struggles.
Families like that of Tawsin find themselves returning home in tears, feeling helpless against the odds.
On Oct 8, bdnews24.com spoke with Liton Mia, a madrasa teacher from Mymensingh’s Tarakanda, at the City Care General Hospital in Dhaka’s Shyamoli, where his 1.3-year-old son Hasan Jamil had been admitted.
Jamil had been admitted to Mymensingh Medical College Hospital on Oct 4 due to fever and respiratory complications, but after two days, the family had to bring him to the private hospital when they could not secure a place at the Shishu Hospital.
Liton said he was initially informed the daily bill would be Tk 4,500. However, the following night, he was handed a bill of Tk 65,000.
"I was told only the ICU charges, but now they are saying I also need to pay for the doctor's fees, medicines, and everything else separately. I have managed Tk 35,000 from relatives and loans, but I have no idea how I will pay the rest," he added.

KEEP YOUR POCKETS FULL
The cost of treating children with conditions like pneumonia, Acute Respiratory Distress Syndrome, or ARDS, Respiratory Distress Syndrome, or RDS, and other respiratory issues in private hospitals is exorbitant.
According to doctors, daily bills can range from Tk 15,000 to Tk 20,000, excluding medication.
Ashis Kumar Chakraborty, managing director of Dhaka’s Universal Medical College Hospital, provided insight into the treatment costs for such children.
Speaking to bdnews24.com, he explained the expenses largely depend on the type of illness.
He said, “If ventilation is required, daily costs, excluding medication, can amount to Tk 15,000 to Tk 20,000.”
He continued, “If a ventilator is not needed, the costs will be somewhat lower. However, if the child requires more oxygen—5 to 10 litres—the price of the oxygen will also add to the bill. Staying in the hospital for a week can easily lead to expenses of around Tk 100,000.”
“But that also depends on other factors; for example, if an expensive injection is needed, the costs will increase further. You can't blindly estimate how much critical care will cost,” he added.
According to the doctor, “People in Bangladesh do not budget or prepare for medical expenses. The absence of health insurance makes it seem like the costs are overwhelming, but in foreign countries, such treatments are even more expensive.”
“Our problem is that no one considers health issues or saves for medical treatment. Regular health check-ups are neglected. As a result, when a sudden illness strikes, families may have to sell their homes. Health insurance is crucial,” he concluded.

WHY SO MUCH PATIENT PRESSURE IN DHAKA?
There are no separate facilities in Upazila health complexes for treating children suffering from respiratory diseases. The facilities available in district hospitals and general hospitals are far from sufficient to match the demand. As a result, such children are often referred from Upazila to district hospitals and from district hospitals to Dhaka.
Upazila health complexes have 50 beds, while general hospitals in the districts have 250 beds, and district headquarter hospitals have 100 beds.
Gazi Md Rafiqul Haque, the health and family welfare officer of Melandah Upazila in Jamalpur, gave an idea about the state of medical care for children with such diseases at the Upazila and district levels.
He told bdnews24.com: "There is no separate ward for children in health complexes. Female children are placed in the women’s ward, and male children are put in the men’s ward for treatment.
"When children come in with respiratory issues, we treat them in the general ward. We have an oxygen line, and if more oxygen is needed, we provide cylinders."
Civil Surgeon of Jamalpur Md Fazlul Haque told bdnews24.com that the 250-bed General Hospital has 32 NICU and Special Care Newborn Unit, or SCANU, beds. There are 24 regular beds equipped with oxygen facilities. On Saturday, 208 children were admitted there.
"There are no separate facilities for children at the Upazila level, but they do exist at the district level. In the NICU, each bed is meant for one child, but often multiple patients share a bed. In reality, we receive five to seven times the number of patients we can accommodate. When there's no space left, we send them to Mymensingh."

WHERE IS THE SOLUTION?
Prof Mesbah Uddin Ahmed, convener of the Bangladesh Pediatric Association, or BPA, told bdnews24.com that everyone shares responsibility for failing to develop a proper system for treating children with respiratory diseases in public hospitals in Bangladesh.
"From the children's hospital to Dhaka Medical [College Hospital], BSMMU, or any other hospital, and finally back home. If they are lucky, the child will survive; if not, the child will return to Allah."
So what needs to be done to solve the shortage of beds in public hospitals for treating such children? Pediatrician Mohammad Shahidullah offered: "The number of beds with oxygen support needs to be increased so that no child is turned away from the hospital."
Prof Mesbah Uddin added, "The load is massive, but the health sector budget is very low. It is difficult to provide such treatment to every child with this budget. The government must take the lead in solving this problem, but it doesn't seem like the government is very committed."
bdnews24.com was unable to get a response from the Directorate General of Health Services, or DGHS, on this matter. When contacted, the new Director General Md Abu Zafar did not answer his phone.











